Contributions Summer 2020
Digital health response to COVID-19 in Burkina Faso
Like most West African countries, Burkina Faso’s health system suffers from significant gaps that reduce its ability to respond effectively to epidemics. The number of COVID-19 pandemic cases in country has slowly but steadily progressed and is now at 895 (as of June 16th), mainly centred in the
country's two major cities, Ouagadougou and Bobo-Dioulasso.
In order to support the fight against COVID-19, Terre des hommes Foundation (Tdh) has implemented a series of activities leveraging
IeDA (the Integrated e-Diagnostic Approach), a digital health solution deployed in over 1,100 Burkina Faso healthcare facilities in rural areas. IeDA is an e-health solution built on the WHO-UNICEF clinical protocol for children under 5 years old and installed in tablets used by healthcare workers. The solution was co-created by Tdh and the Ministry of Health (MoH) of Burkina Faso in order to improve quality of care at the primary care level and to save children’s lives. Tdh has recently enriched IeDA with new features, including integration of point of care tests, creation of interactive web maps and dashboards, artificial intelligence analyses, and perinatal health digitalization, among others. An external evaluation shows a significant improvement in the quality of care thanks to the digital solution, an increased diagnostic accuracy and a reduction of maintenance costs compared to paper version. Over 6 million consultations have been performed by IeDA to date.
To support Burkina Faso’s pandemic control efforts, Tdh developed and built the following digital solutions into IeDA:
Decision aid-tool for triage: The Corona Triage App, which Tdh created in collaboration with the Burkina Faso MoH and UNICEF, helps healthcare workers to identify and follow up possible COVID-19 cases (launched on June 1st).
Communication awareness and counselling: During child health consultations, IeDA prompts healthcare workers to provide COVID-19 awareness messages, such as on hygiene practices and social distancing, to the parents or child caregivers.
Capacity building: Through a set of e-learning modules uploaded in IeDA tablets, healthcare workers learn about: COVID-19 Diagnosis and Epidemiology, Pregnancy and COVID-19, Infection Prevention and Control, COVID-19 and Surveillance, and COVID-19 in Children
These specific COVID-19 digital solutions have been deployed in all healthcare facilities where IeDA is available, equalling coverage of two-thirds of the country.
Data generated through IeDA’s 200,000 monthly child consultations is an additional resource for addressing COVID- 19, as it offers an opportunity to monitor the pandemic’s impact on routine health services. A growing concern is that the impact caused by the disruption of routine health services, and changes in health seeking behaviour could be much higher than COVID-19 itself, particularly among children. The initial analysis of a large IeDA dataset from rural zones suggests that COVID-19 has not yet impacted the use of health care services for children under five in Burkina Faso. This result might be explained by a delay in the pandemic spread, especially in rural areas. Access and analysis of reliable and timely data will be essential for ongoing monitoring of the pandemic’s progression in the country and for supporting quick response to any arising challenges that could impact the provision and use of health services, particularly among the most vulnerable populations.
As the virus continues to spread, digital health offers great potential to support Burkina Faso and other countries to improve their national health surveillance and epidemic control efforts. While digital health solutions will not end the pandemic, they represent an additional weapon in the fight against it.
Contact
Riccardo Lampariello
Terres des hommes Foundation
RLA@tdh.ch

Albania
A new initiative in Albania supports young researchers to conduct operational research in health
Albania faces lack of evidence in primary health care and public health that creates a gap between policy making and planning processes and operations to undertake to gain health benefits. There is lack of human resources and capacities to conduct operational research and insufficient financing opportunities.
Therefore, Health for All Project (HAP) is supporting young researchers under the initiative ‘Operational research in health 2020’. The main two objectives of the initiative are: (I) to provide funding opportunities for conducting operational research on different aspects of health services in Albania with a focus on primary health care and public health and (II) strengthen research capacities of young researchers through training and coaching during implementation of operational research activities.
HAP invited young researchers to apply for financial support for operational research in domains of health such as human resources in health, NCDs as a public health issue, health information system in primary health care and beyond, quality of primary health care in Albania etc. 45 proposal were submitted by applicants of different backgrounds: medicine (31%), public health (25%), technical medical sciences (22%), economy (13%) and social sciences (9%). The average working experience of applicants was 6.4 year, and gender representation was in a range of 89% female and 11% male.
An independent selection board composed by senior academics and researchers, representatives of four Universities and Research Institutions in Albania evaluated the applications and selected the first cohort of 11 young researchers (
click here to download the list of wining proposals). The young researchers will attend courses on research related topics and will start the operational research work in the upcoming weeks.
The ultimate goal of HAP is to enhance research capacities in Albania and create new opportunities and models for funding and conducting operational research activities in the country, thus increasing the offer of sound and systematic evidence-based data that would provide to policymakers reliable and efficient knowledge on the health system.
Contact
HAP Team: info@hap.org.al

Albania
Digitalization in times of COVID-19: insight from HAP supported activities in Albania
“There was little information in the first days we faced COVID-19, especially in early March. Everyone, patients, family members, friends were asking us to provide information about this new disease” - says Dr. Artenca, a family physician in Tirana. Several other primary health care professionals felt the same as Dr. Artenca and began searching for updated information on COVID-19 on the official websites of health institutions, both national and international. They soon encountered two main challenges: first, the materials focused mainly on first-line professionals dealing with the identification and treatment of COVID-19 suspected/confirmed individuals (epidemiologists, infectious disease specialists, pneumologists, etc.) and second, most of the materials were in English which made it difficult to consult them and convey important messages to others, especially to the general public.
Aware of this need for information, the Health for All Project (HAP) immediately began elaborating educational materials for COVID-19 infection in Albanian, targeting PHC professionals as well as the general public, based mainly on data from the WHO and the Center for Disease Control and Prevention (US and Europe). The digital learning content, mostly as a powerpoint with an audio explanation attached, is delivered on the HAP website. “On the HAP website we found answers to many questions we received from patients for instance on self-isolation and self-quarantine, advices to pregnant women and new mothers. It was great to access materials that can be easily read and understood by the general public thus making it easier to disseminate them” - says Dr. Xhovana, family physician at Kuman HC (southern Albania). Sokol, a nurse at Zerqan HC (northern Albania) and his colleagues have followed-up a COVID-19 infected patient and tells how specific topics have been of help to him: “As expected, the patient himself, his family and his contacts panicked, so HAP materials related to stress management during COVID-19 helped us a lot in providing the necessary practical advices.”
With Albania exiting lockdown and training activities being allowed, PHC teams have planned a series of trainings through Peer Groups using the full set of training materials developed by HAP on COVID-19 infection prevention and control. The trainings are being recognized as a continuous medical education activity and accordingly accredited by the National Center for Continuing Education (NCCE).
After the first clash with COVID-19, PHC professionals need to learn to "co-exist" with the risk of the new disease. In these conditions, they highlight the need for a guide/tool to improve the quality of remote consultation as well as communication and information platforms with patients, for COVID-19 and not only. In this context, HAP is working furthermore on developing a quick guide for remote consultations of patients affected by chronic non-infectious diseases and it is planning to set up an electronic system for consultations appointments to the health centers. HAP is also working with Swiss TPH and probably Unisanté to adapt the CoronaCheck platform in the Albanian context and make it available to the general public.
Related resources
http://www.hap.org.al/en/homepage-covid-19/
Contact
HAP Team: info@hap.org.al

Kosovo
AQH’s virtual working mode during COVID-19
Our communication and collaboration with colleagues, partners, and stakeholders has gradually transitioned to virtual platforms for meetings, training session and quality improvement measures. E-solutions to reach partners as well as patients are increasingly in demand.
Highlights for this month:
Awareness raising communication materials reaching a large audienceSince the beginning of the pandemic, AQH has focused on communicating intensively with the public through social media platforms and Television channels, while creating trend-setting campaigns together with the Ministry of Health and National Institute of Public Health. Preventive and protective measures, living with social distancing, impact of COVID-19 on people living with NCD’s, minimizing infection risk when visiting restaurants, shops, were some of the topics tackled on video materials aiming to raise awareness among the public.
Telephone consultations of nurses with chronic patientsA very innovative approach that was embraced by our project is the use of telemedicine approaches for chronic patients. Rather than having to visit medical facilities, patients diagnosed with diabetes and hypertension have the possibility to get advice and answers to their questions through telephone consultations with their nurses. Amongst others, this also avoids additional risks of virus infection through close contact with other patients.
Health Management distance trainingCurrently, the most important part of the discussion in the health sector remains infection prevention, social distancing and the availability of personal protective equipment. However, AQH continues to strengthen quality management processes by distance training activities.
Online training sessions for infection prevention and controlInfection prevention and control measures are deservedly high on the agenda for patients, nurses and decision makers. AQH organized online training sessions covering this topic with doctors and nurses from 12 municipalities in Kosovo.
Health education campaign on Second hand smokingThe AQH health education campaign focused on “second hand smoking” is implemented virtually in cooperation with National Institute of Public Health.
For further details on our AQH activities during this period please have a look at our
most recent newsletter.
Related resources
https://www.facebook.com/AQHproject/
Contact
Merita Stavileci
Senior National Programme Officer at Swiss Cooperation Office in Kosovo
merita.stavileci@eda.admin.ch
Moldova
Adapting a Chronic Disease Self-Management Programme to the realities of the COVID-19-induced lockdown
In 2019, the Healthy Life Project piloted the Chronic Disease Self-Management Programme (CDSMP) in 5 pilot communities in parallel with other activities aiming to increase health literacy among the population regarding behavioural risk factors (food consumption patterns, tobacco use, alcohol consumption and physical activity) of NCDs, health care seeking behaviour and to promote a healthy lifestyle. During the piloting of CDSMP 63 patients with chronic conditions benefited from the 6 weeks programme centred on individual goal-settings for small lifestyle changes. Building on the positive, evidence-based results from the pilot intervention, the project had prepared to expand the CDSMP to 20 more villages and just concluded the training of CDSMP facilitators when lockdown restrictions were imposed. The lockdown meant group-based activities and face-to-face interactions became impossible. The Healthy Life Project creatively adapted to the situation by relying on the widespread use of messenger applications and telephone discussions. For 6 weeks, 36 facilitators held weekly video-based group chats with their 279 CDSMP participants using Messenger or Viber. While the first 2 sessions were mostly devoted to sharing and discussing COVID-19-related health information and prevention measures, the subsequent sessions progressively returned to following more closely the pre-set CDSMP workshop agenda. This included a focus on healthy nutrition, pain management, medication administration, and physical activity – all of which were accordingly adapted to the new realities of the lockdown situation. Preliminary qualitative feedback from the participants indicates that this approach provided an important mental health support in the early days of the pandemic. In particular, it helped to address participants' anxiety, depression, and feeling of isolation amongst risk groups of the elderly living with NCDs in remote communities, while providing an innovative vehicle for sharing accurate health information.
Links to related resources
Barlow, J. H., Wright, C., Sheasby, J., Turner, A., & Hainsworth, J. (2002). Self-management approaches for people with chronic conditions: a review. Patient Education & Counseling, 48(2), 177–187. Brady, T. J., Murphy, L., O'Colmain, B. J., Beauchesne, D., Daniels, B., Greenberg, M., Chervin, D. (2013). A meta-analysis of health status, health behaviors, and healthcare utilization outcomes of the Chronic Disease Self-Management Program. Preventing Chronic Disease, 10, 120112.http://doi.org/10.5888/pcd10.120112 Haslbeck, J., Zanoni, S., Hartung, U., Klein, M., Gabriel, E., Eicher, M., and Schulz, P. (2015) Introducing the Chronic Disease Self-Management Program in Switzerland and German-speaking countries: findings from a multiple methods study. BMC Health Serv Res, 15, 576. 10.1186/s12913-015-1251-z Lawn, S., & Schoo, A. (2010). Supporting self-management of chronic health conditions: common approaches. Patient Education & Counseling, 80(2), 205–211. http://doi.org/S0738-3991(09)00496-0 [pii] 10.1016/j.pec.2009.10.006 Montori, V. M., Gafni, A., and Charles, C. (2006) A shared treatment decision-making approach between patients with chronic conditions and their clinicians: the case of diabetes. Health Expectations, 9,1, 25–36. 10.1111/j.1369-7625.2006.00359.x Taylor, S. J., Pinnock, H., Epiphaniou, E., Pearce, G., Parke, H. L., Schwappach, A., Sheikh, A. (2014). A rapid synthesis of the evidence on interventions supporting self-management for people with long-term conditions: PRISMS – Practical systematic Review of Self-Management
|
Contact
Dr. Valeriu Sava
National Program Officer Health, Swiss Cooperation Office in Moldova
valeriu.sava@eda.admin.ch
Rwanda
Action Research on Horizontal Learning Process (HLP) for the prevention of child stunting in the Western Province of Rwanda
In spite of significant improvements in the health sector service delivery, the incidence of chronic malnutrition (stunting) among children in Rwanda remains high, affecting 38% of children under five and more than 50% for children aged between 20-30 months, the Western province being among the most affected (1). Childhood stunting is one of the most persistent health and development problems of the country. Thus, the Government of Rwanda has placed stunting high on its priority list.
What is stunting? Children are defined as stunted, or chronically malnourished, if they are shorter compared to their age. Stunting has multiple causes, including poor nutrition, repeated infections and inadequate psychosocial stimulation. It has severe short-term and long-term health and physiological consequences, such as impaired brain and physical development, low performance at school and lower prospects as an adult. Optimal nutrition during the first 1,000 days of life can have a lasting impact on a child’s growth, learning, and future productivity (2).
The Swiss Agency for Development and Cooperation (SDC) has provided support for the Rwandan health sector since 2002. As part of this support, a participatory action research was conducted between 2017 and 2020 to explore some of the causes of chronic child malnutrition and to support knowledge sharing among the primary caregivers, the parents and community health workers.
Targeting the Western Province of Rwanda, the research involved 2700 children under 2 years of age with their respective caretakers from 90 villages, 90 community health workers, the nutritionist of the 6 health centres, the district and health centre authorities and the entire community. It aimed at exploring the causes of chronic child malnutrition and innovative ways to overcome them by engaging parents, caretakers and community health workers in sharing their innate knowledge and best practices on nutrition and hygiene for children, and stimulate learning and behaviour change.
The project was designed around two parallel interventions: 1) quarterly, facilitated growth monitoring of children, and 2) community-based “Learning Together” sessions.
With, the growth monitoring intervention, measurements results and nutritional status of the children were systematically explained to mothers to improve interactions and communication between health providers and caretakers. Children suffering from severe, chronic or acute malnutrition were referred to the health centres and followed-up by community health workers.
The “Learning Together” sessions consisted in community-based meetings on a monthly basis. During these sessions, 30 caretakers per village met to share knowledge and good practices related to nutritional and hygienic behaviors influencing child health. The sessions were interactive, participatory and based on a horizontal learning approach. Learning together sessions were moderated by local CHWs.
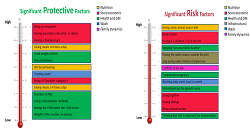
What is it Horizontal learning? The horizontal learning approach is based on the assumption that people have innate capacities that can be catalysed through peer support for their own and their children’s wellbeing. Horizontal learning focuses on three main concepts:
Appreciate – To recognize that everyone has the potential to contribute positive ideas, regardless of their circumstances;
Connect – Appreciation from heart helps to remove the distinctions that separate people;
Adapt/Replicate – Start with the ideas that work, and replicate them through exposure to the local context (3).
Achievements and findings of the Project:
The combination of the two interventions had a positive effect on the nutritional status of children. The percentage of severely stunted children significantly decreased in age category 12 to 18 months, and the age-dependent stunting progression was slower among the children participating in the project compared to the control group.
The action research was positively received by the community; more than 98% of the caretakers participating in the project remained engaged until the end of the intervention by participating at every leaning together and growth monitoring session. Caretakers learned how to read and interpret the growth-monitoring curve, and developed a better understanding of the causes and consequences of stunting, contributing to increase the visibility of the issue.
The community health workers received valuable capacity building skills and improved their ability to share their knowledge with the community.
The project also demonstrated that engaging parents, caretakers and CHWs to share their innate knowledge and best practice experiences using a participatory approach creates learning, stimulates behaviour change and improves the nutrition status of the target population.
Overall, the two interventions contributed to increase the visibility of stunting among caretakers and communities, while emphasizing locally appropriate good practices, which can help, prevent stunting.. There was overall a high level of appreciation of the interventions at all levels, from the caretakers to the District and Provincial stakeholders, suggesting the acceptability of the approach.
Conclusion: This action research demonstrates that a participatory approach such as Horizontal Learning can efficiently complement and reinforce a conventional capacity building approach normally used at the community level. While traditional capacity building assumes that there is a lack of capacity that has to be addressed by experts, the horizontal learning approach starts with the assumption that there are existing capacities in the community which can be mobilised through peer exchange.
Regular growth monitoring is a successful strategy to reduce chronic malnutrition in the population and to increase caretakers’ awareness of of stunting.
Finally, the project added to the evidence base on the complex causes of stunting and suggests that the fight against chronic malnutrition needs to be addressed through a multi-sectorial approach.
Links to related resources
(1): National Institute of Statistics of Rwanda (NISR) [Rwanda], Ministry of Health (MOH) [Rwanda], and ICF International. 2015. Rwanda Demographic and Health Survey 2014-15. Rockville, Maryland, USA: NISR, MOH, and ICF International. (2):
https://thousanddays.org/ (3): Shams Uddin Ahmed, Santanu Lahiri, Horizontal Learning Program in Bangladesh: The Program Framework, November 1, 2011 – October 31, 2015. |
Video of the Action research:
https://www.youtube.com/watch?v=osmPdDtjt48&feature=emb_logo
Contact
Theoneste Twahirwa, Senior National Program Officer in Health
SDC, Rwanda
theoneste.twahirwa@eda.admin.ch
Adriane Martin Hilber
Scientific Collaborator and Postdoc at Swiss TPH
adriane.martinhilber@swisstph.ch

Tanzania
Supporting the call centre for the national COVID-19 hotline in Tanzania
The first COVID-19 infection case was reported in Tanzania on 17th March 2020. Since then the Health Promotion and System Strengthening Project (HPSS) funded by the Swiss Agency for Development and Cooperation (SDC) and implemented by Swiss TPH was engaged in supporting the Government of Tanzania in the implementation of its COVID-19 Emergency Response Plan. HPSS reallocated an amount of up to CHF 222’000 to support the GoT in the COVID-19 response, out of which CHF 25’000 is dedicated to supporting Zanzibar. The project’s support is mainly provided on establishing a modern call centre and on awareness raising and communication with the distribution of 100’000 posters and broadcasting of radio spots.
On 8th of May the Minister of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) Hon. Ummy Mwalimu launched the new “Afya Call Centre” for the Corona virus response hotline “199”. HPSS jointly with IMA World Health and UNFPA supported the building of the hotline’s infrastructure and expanding of its capacity.
The Call Centre was designed in a way that it can accommodate the needs of the country to respond to the pandemic: address community concerns, myths and lack of knowledge, as well as provide guidance regarding testing, care and treatment of COVID-19. The technical features of the Call Centre include an Interactive Voice Response (IVR) System for automated answers in order to free time for the operators for attending to the remaining calls. The IT system can technically accommodate 500 concurrent calls, and has the possibility to be connected with stations in other cities across Tanzania. When the Government decides to establish other health related hotlines there will be no need of procuring a new system.
The Afya Call Centre operates 24 hours a day with two shifts of 40 operators each. The Ministry of Health will change the shifts to 8 hours after finalisation of the recruitment processes of all 120 operators.
Since establishing the new IT system the call centre substantially increased the capacities of the Ministry of Health to receive and respond to questions of the citizens on the COVID-19 health issues. The newly launched Call Centre is attending to between 75 to 82 percent of the incoming calls.
|
Date |
Total calls incoming |
Nr. of calls attended to by operators |
Nr. of calls attended to by IVR |
% of calls attended to |
% of calls not attended to / timed out | |
Previous call centre (TTCL) | | | | | | | 16.03.2020 | 4'944 | 179 | - | 4% | 96% | | 17.03.2020 | 20'495 | 1'111 | - | 5% | 95% | | 18.03.2020 | 29'450 | 1'715 | - | 6% | 94% | | 09.04.2020 | 52'414 | 5'709 | - | 11% | 89% | |
Afya Call Center
1) | | | | | | | 09.05.2020 | 3'752 | 1'373 | 1'714 | 82% | 18% | | 14.05.202 | 37'053 | 11'430 | 16'941 | 77% | 23% | | 15.05.202 | 36'794 | 11'393 | 16'784 | 77% | 23% | | 20.05.2020 | 62'401 | 18'458 | 28'088 | 75% | 25% |
- Except for 20.5.2020, data for other days are for 12 hours only
Source: MoHCDGEC
|
The support in the establishment of the Call Center has enhanced the ability of the government to use a sustainable communication channel with the population both for the COVID-19 public health crisis, but also for future other related topics, e.g. on general health, or gender based violence health related topics.
Related resources
Contact
Jacqueline Matoro
National Programme Advisor for Health, Swiss Cooperation Office in Tanzania
jacqueline.matoro@eda.admin.ch

Tajikistan
Experience in health management training at district PHC level
In Tajikistan, further development of Primary Health Care (PHC) based on the principles of family medicine is one of the key priorities of the National Health Strategy. SDC’s “Enhancing primary health care services in the Republic of Tajikistan” places an important focus on building management and planning capacity for PHC at district level.
Under the oversight of the Ministry of Health and Social Protection, in 2015 a curriculum and practical, modular course for PHC managers was developed by the Post Graduate Medical Institute in the Republic of Tajikistan (PGMI) and Swiss TPH.
Key features of the course are: a) in-depth practical focus, a limited number of hours of theoretical lectures in Dushanbe city with the bulk of the course takes place in the PHC managers workplace with mentoring by the institute's trainers; b) use of innovative teaching methods; c) application of modern concepts for PHC system that take the real situation in the district into account and emphasize practical problem solving.
The course curriculum comprises 10 training modules, in total 1,716 training hours, including topics that are completely new for Tajikistan - modules on Management in practice, business planning, community engagement, infrastructure management and planned preventive maintenance, etc.
The duration of each training module is 4 weeks: the first week is at PGMI in Dushanbe; the second week - self-learning of trainees at their workplace; third week - On Job Training and mentoring by the PGMI trainers at the rayon level; and the fourth week is the assessment time, when the trainees provide their completed, practical assignments.
Since June 2015, 3 iterations have been successfully completed, and since February 2020 the fourth iteration is ongoing. In the first two iterations, the participants were only supported by the EPHC Project pilot districts, and in the 3rd and 4th iterations, the participants of pilot rayons of the Aga Khan Health Services (AKHS) from the Rasht region also started to take the course.
The main participants, district PHC managers and their deputies are trained and receive a diploma “Public Health Manager”. Also, specific PHC management staff are involved to the separate modules depending on their work profile (IT/business planning specialists, HR specialists, accountants, head nurses, district and oblast HLSC staff) and receive a certificate. Team training increases the effectiveness of the program.
In 3 iterations, heads of the oblast PHC department (3 people) and 23 PHC Managers and their deputies have been trained, and 69 specialists from district PHC management team attended in the thematic modules depending on their work profile.
The current iteration was ongoing as restrictive measures were introduced to prevent the transmission and spread of Coronavirus infection - COVID 19. To ensure the continuity of the learning process and to protect participants and trainers to be infected by Coronavirus, PGMI took the initiative to start running the course online using video conferences,
online
teaching of 2 modules
Modules “Knowledge Management” and “Human Resource Development”, and remote online support the trainees in their field .
Technical issues in the districts could be overcome, and PGMI operated from the MoHSP’s
Resource Information Center, through Zoom.us/ru program for conducting the classroom part of sessions (lectures, seminars and workshops) in the format of video conferences in real time.
The participants were informed in advance about the dates and time of the training Module, presentations on the topics were sent in advance to the participants. Also, a code and password for access to the videoconference were sent to all participants. PGMI trainers were actively involved in the process of organizing and conducting classes. Despite the rapid transition made, all lectures were conducted in an interactive way with the active involvement of participants in the learning process. Most managers actively contacted at the defined time and date.
PGMI is considering to maintain the new distance learning modalities for greater efficiency as they move forward with the course, and start to engage other donors in -country to support PHC managers to take the course.
Contact
Dr. Gulara Afandiyeva, Head of Swiss TPH office
in Tajikistan
gulara.afandiyeva@swisstph.org
Dr. Muazamma Dzhamalova
National Program Officer Health, Swiss Cooperation Office in Tajikistan
muazamma.dzhamalova@eda.admin.ch

Ukraine
Online course ‘Medical Assistance during COVID-19 Pandemic’ in two editions for primary health care doctors, nurses, and other medical professionals
Addressing the challenge of access to updated, reliable and evidence-based information on COVID-19, the Ukrainian-Swiss Project ‘Medical Education Development’ in cooperation with the Public Health Center of Ukraine introduced a serries of online-course ‘Medical Assistance during COVID-19 Pandemic’.
The content partner of the first edition of the course was the Academy of Family Medicine of Ukraine which selected the most professional and well-known lecturers to deliver the following 8 lectures in Ukrainian (available on Youtube channel of the Project):
Coronavirus disease: basics of infection control in outpatient practice. Home visits
Newborn patronage during the COVID-19 pandemic
Telephone Consultations: Algorithms for Successful Communication during the Pandemic
Counseling of patients with panic attacks during the pandemic: the role of family doctor and nurse and nurse
Vaccination during the COVID-19 pandemic
Coronavirus and cardiovascular disease: international guidelines
Algorithms for Pregnancy, Childbirth and Newborns in Coronavirus Disease
Coronavirus disease and immunodeficiency states
Coronavirus disease and chronic lung pathology.
So the lecturers are able not only to provide information based on international guidelines and WHO recommendations but also to clarify the most common concerns and answer the most urgent requests, the project collected over 1000 questions form medical practitioners to be addressed during the online-lectures.
The second edition of the course was developed by the medical network ‘Dobrobut’ (a private clinic which is treating patients with COVID-19) and the Public Health Centre of Ukraine. This course was based on practical experience analysed by doctors and nurses, administrative staff of the partner institutions. This time not only lectures were delivered but also practical sessions with demonstration on how to put means of individual protection, how to use ventilators and ensure safe patients flows.
As of 10. June 2020 for the first edition of the course 7056 medical professionals were registered and for the second edition – 1550 specialists.
This course is recognised as an official continuous professional development course and available until 1. August 2020 on the educational portal of the Public Health Center of Ukraine.
The spread of COVID-19 brought a number of challenges to health care systems all over the world. Ukraine faced this pandemic being in the middle of a health care reform – one step from the start of its second stage: financing of specialized care. At the same time, almost monthly executive personnel changes in the health ministry did not allow to implement sustainable efforts to protect health care professionals, patients; to provide reliable guidelines on prevention and treatment of COVID-19; to introduce streamlined and trustworthy communication from the Ministry to ensure fair patients flows and answer those questions which appeared day by day. As lots of medical professionals in Ukraine do not speak English, this complicates the access to international protocols and recommendations, and further requires additional efforts for translation and clarification. Therefore, the joint efforts of the Project and
Contact
Martin Raab
Senior Public Health Specialist and Project Manager
Head of the Health Technology & Telemedicine Unit
Swiss Centre for International Health
martin.raab@swisstph.ch

Bern
Assuring quality of medicines – the role of development partners
Addressing the challenge of access to updated, reliable and evidence-based information on COVID-19, the Ukrainian-Swiss Project ‘Medical Education Development’ in cooperation with the Public Health Center of Ukraine introduced a serries of online-course ‘Medical Assistance during COVID-19 Pandemic’.
The following principle will help apply the same requirements and international standards for the procurement of essential medicines and other healthcare commodities:
All essential medicines purchased with donor funding must be quality-assured. They are quality-assured when they are either pre-qualified by WHO (http://www.who.int/medicines/publications/essentialmedicines/en), or approved by a regulatory agency upon which WHO relies for its pre-qualification assessment. This is the case of Swissmedic, the Swiss Agency for Therapeutic Products that assesses the manufacturing practice, enforces quality assurance standards in the case of non-compliance and also surveys the quality of the products after approval once it is on the market.
It must be also documented that the product is suitable for an intended geography (e.g. language/labeling; heat stability).
Under exceptional circumstances and on a defined interim basis of 12 months, products may be qualified by an Expert Review Panel convened by WHO if no quality assurance assessment is available. For instance, The Global Fund uses this mechanism while waiting for the product to be pre-qualified by WHO.
As a last resort, products may also be procured from accredited sources such as internationally approved wholesalers.
All products purchased with donor funds must also be approved by the national medicines regulatory authority.
Donors expect all bids to reflect these principles, and also require adherence to them by partner country governments when they directly purchase medicines.
Related resources
Contact
Alexander Schulze
Co-Head Global Programme Health, Swiss Agency for Development and Cooperation
alexander.schulze@eda.admin.ch